








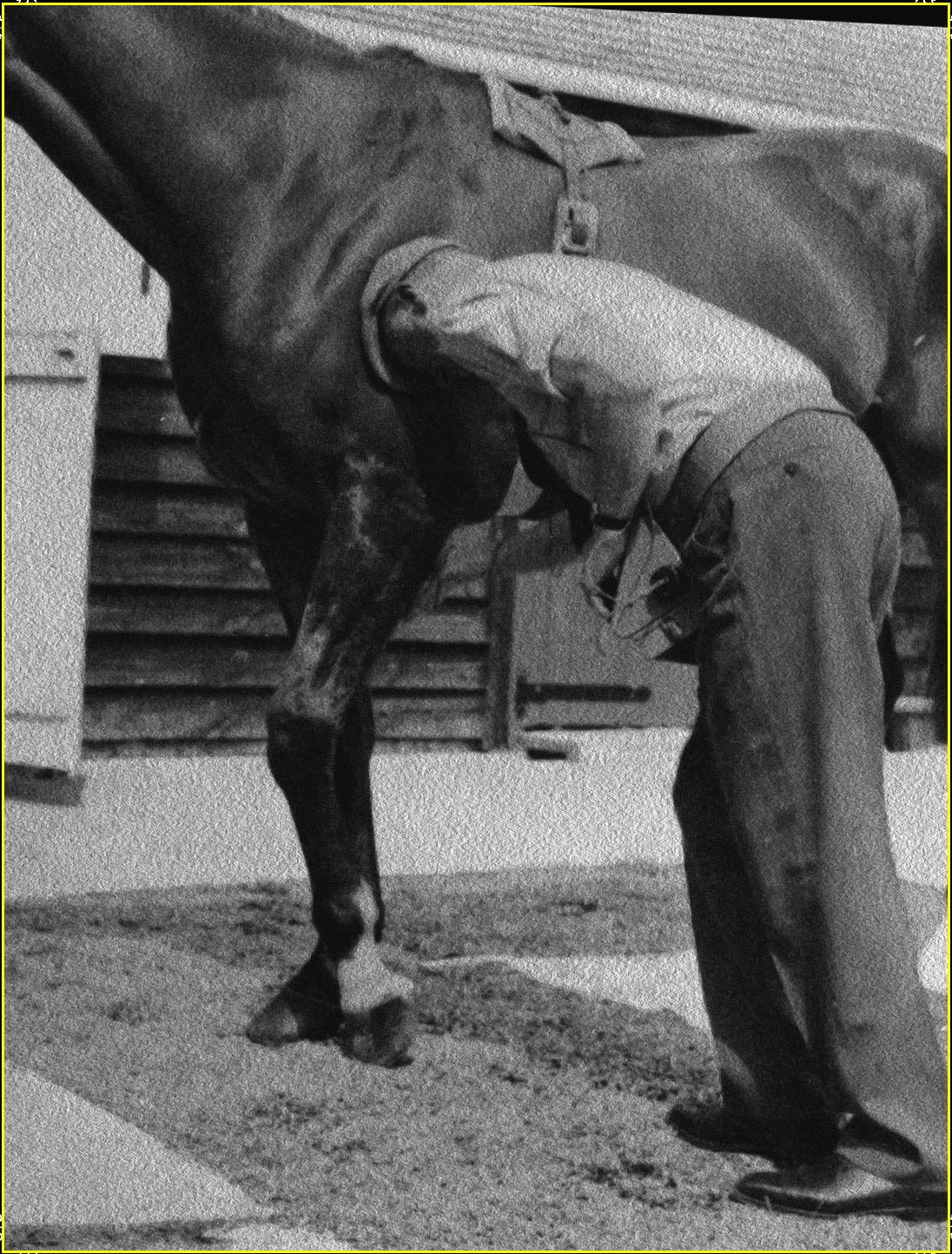

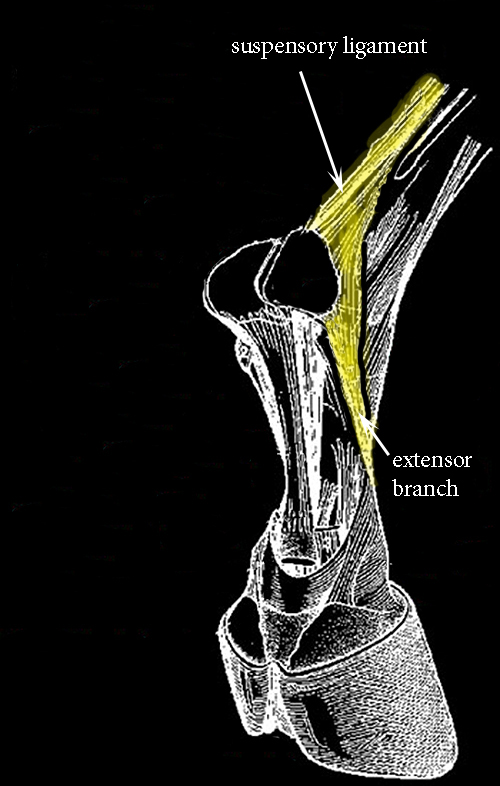






















The above photo depicts the first test one should use to palpate (feel) for suspected suspensory ligament damage. Lift the suspected leg up, and take your fingers and carefully finger-pinch down the length of the suspensory ligament--pinching on each side of the ligament as you go down looking for a response from your horse for soreness. Knowing where the suspensory runs is vital in knowing what structure to put your fingers on! The suspensory can be felt below the superficial and deep flexor tendons, running next to the cannon bone, alongside the sesamoids. Know the structures of your horse's leg well! Pinch carefully down the length of the ligament from its origin just below the knee, down to where it branches off into two structures alongside the sesamoids (a common area of injury as pictured to the right) on each side of the ankle. Flexing the ankle as a whole can also often elicit suspensory pain and may be an indication, though when flexing the entire ankle joint; of course, other structures will be involved along with the suspensory apparatus. In more advanced cases of ligament injury, it will be obvious by simple observation that the ligament is involved. Injury can occur anywhere on the ligament, but the more common site is near the ankle where it bifurcates along each side of the sesamoid bones and this specific region location will be the main focus of this page.
First off, what is the cause of suspensory injury in most cases though one will always run into freak accidents of one sort or another when dealing with horses? I have found that most suspensory ligament strains occur on the racetrack as mostly a function of the flexor muscles and tendons failing to do their job for one reason or another and letting the suspensory take-over more weight-bearing work than it was designed to handle while at the same time landing on uneven ground. With the fatigued flexor muscles not able to fully assist in the snap-off of the planted, unlevel hoof, a tear in one of the suspensory branches can occur. A second reason can also occur and it is a result from a secondary soreness. If your horse is off somewhere else in the affected leg, then he may try to land unevenly to take the pressure off of the pain he is feeling resulting in his hoof landing unevenly.
The lower legs of the horse is supported by basically three structures to prevent over-extension of the ankle joint:
1) suspensory ligament (interosseus) which runs from just below the knee to inserting on each side of the sesamoids and then further down toward and inserts on the 1st phalanx in the fetlock. It catches the body weight in motion aided by the flexor tendons. On hoof impact, it stretches like a spring until mid-stride (cannon bone vertical) then during the second half of the stride, the suspensory shortens like a stretched rubber band, propelling the fetlock back up again.
2) deep and superficial flexor tendons that are extensions of the forearm's flexor muscles and insert on the phalanx bones of the fetlock. They are both instrumental in assisting the suspensory in its weight bearing activities.
If for some reason, the flexor muscles of the forearm or rear leg are not working normally in keeping weight from over-extending the ankle joint of which fatigue is often the major culprit, then the flexor tendons will often fail to support the suspensory in its job resulting in suspensory damage. So to prevent suspensory damage, one races a fit horse that is unlikely to become so fatigued as to damage that ligament. There may often be flexor muscle damage in conjunction with the injured suspensory that may go unnoticed and should be treated simultaneously. Plus, to prevent future damage or re-injury, one must make sure your horse is conditioned and "fit" which is often the last thing many trainers have a tendency to do when trying to protect a suspensory injured horse or any injured horse for that matter!
But be that as it may, let's presume we are faced with treating a suspensory injury. One has to stimulate proper healing. It will not happen on its own, certainly not by the common veterinarian prescribed procedures of stall rest and bute. Stress is required to be exerted on the damaged ligament in order for the body to know how to reinforce it. Movement is required to facilitate the blood and lymph pumping action. Stall rest will not tell the horse's body anything other than how to heal a damaged suspensory to withstand STALL REST. So if you want a horse to heal a healthy ligament or tendon for STALL REST than you are doing the right thing following a vet's advice of stall rest. If you want a horse's suspensory strong enough to be useful in a racing environment, then you most certainly will fail with a stall rest regime. I dislike bute and all other anti-inflammatories or pain relievers. Occasionally, they have their place, but on the whole they hurt solid systemic healing and they mask the true condition of the horse making things more difficult for the trainer to monitor progress.
Pain is good, particularly a little pain. So don't get excited if your horse is nodding at a walk or trot. It is unlikely a walk will re-damage any suspensory tissue injury. The same thing can be said for a trot and even a canter, further on into the healing time slot of a suspensory. You need this stress of movement of ligament strain in order to tell the horse's body how to best heal in the most logical and strongest fashion, the desired, straight up and down, longitudinal fibers. Some stall rest is ok when very first injured, but don't go overboard. Let the horse tell you when he needs more exercise. There is no clean cut, cook book prescription on how to give all horses the same exercise. So don't ask. Just understand the principles and know the faster you get the horse moving the better off you and he will be. The Brit, Charles Strong writes that an injured horse should probably be "moved" on the same day as the injury or at least soon afterwards!
I will give my opinion, based on successfully racing a few horses with suspensory damage. Thankfully, that has been few and far in between! I have very little respect for vets when it comes to tendon and ligament treatments. They are good about sticking needles in, pushing pain/anti-inflammatory pills, pushing expensive procedures to pay for expensive instrumentation and most of all, prescribing prolonged stall rest. I wish I could say they were a lifesaver in my career of training race horses, but they were not. I would like to have a dollar for every horse they said that would never race again and did exactly that from the hard work of a groom, the expertise of a trainer and, much of the time, simple common sense.
RICE versus MEAT
I am generally not in favor of what many would call RICE (rest, ice, compression, elevation) therapy as employed in the human sector which has often been adapted to the equine world. Rest can cause muscle atrophy and adhesion formation, Compression (bandaging) can cause localized anemia from limiting blood and lymph supplies to the injured part and elevation is not practical in the horse, but likewise is designed to drain the site of healing fluids. The smart sport therapists are leaving the RICE theories behind for what is now known as MEAT (movement, exercise, analgesics, treatment). I agree and have been way ahead of them in this respect. My race horse training mentors of my past, Charles Strong and a couple of hall-of-fame trainers have utilized MEAT and I have as well with great success. I try to avoid the use of bute or any analgesics, but movement and exercise is a MUST in most injuries. However, the sentiment for analgesic use in MEAT is appreciated in that many MEAT followers think exercise is so important that they will use pain killers to stimulate it! I don't and it is not generally needed to my way of thinking! Pain killers only muddle the picture. As I have said before, this type of therapy is a delicate dance of providing just enough movement exercise to stimulate healing without re-damaging the injury. The key is to increase blood circulation and to provide adequate nutrients to the site of injury while at the same time pumping away the by-products of that injury. Without inflammation, increased blood & lymph flow and the equally important action of pumping out the toxins, the injury will not heal properly. Movement increases blood/lymph flow and also tells the system how to best strengthen its regenerated tissue for racing. Rest will never tell the horse's healing system what is needed to strengthen itself except how to stay healthy in a stall. As far as the "T" in MEAT, "treatment", I will discuss this subject toward the end of this page in one concise regime.
Don't get me wrong, some stall rest may be necessary in a very limited way, but that stage often passes very quickly and when I say "stall rest" I still mean therapeutic contraction & relaxation of the proper muscle groups taking place in a stall setting, just not actual work outside of the stall. However, following the advice of the genius, Charles L. Strong, the sooner one starts treating a suspensory or tendon injury the better! Perhaps even the same day! I quite agree! He writes in his book, Horses' Injuries:
"It might be thought that to use this treatment (EMS) so soon after injury might increase the inflammation. Experience in the treatment of horses for some twenty years or more, and humans for over 36 years show that this is not the case. Not even in one single case has it been experienced." He further writes: "There can be no greater mistake than to see what a few days rest will do. In a few days it is remarkable how the escaped blood and lymph can stagnate, the edema stretching the surrounding tissues with the possibility of forming into crippling adhesions, if the rest is continued and absorption does not take place."
He employed an electronic muscle stimulator (EMS) to start contracting and relaxing muscle fibers as soon after injury as possible without actually putting a rider up on that horse to get the same effect. Chances are you will not have an electronic muscle stimulator at your disposal when you need it the most. I suggest you should have one in the tack room as they are as important as any other key piece of tack, but we all have our priorities on what we can afford or need in the barn. EMS units are not only good for treatments, but can be a very useful diagnostic tool letting the trainer know that a certain group of muscles may be sore which otherwise would have gone unnoticed. Useable portable EMS devices can be had second-hand for under $100 on ebay and there are really no substitutes outside of very careful exercise the first few days or week without it. For a more in-depth discussion on electro-medicine and electronic muscle stimulation go to my web-page, Electro-Medicine Part 2 . Just don't try to use the commonly available TENS units as is sometimes done. You want to only employ an EMS capable unit to obtain proper muscle contractions! TENS is designed to numb the nerves, not stimulate muscle tissue.
The suspensory ligament is a very interesting unique structure in that it is thought to have evolved from a muscle, quite different in composition and mechanism from its neighbors, the deep and superficial flexor tendons. By rignts, it should never be called a "ligament", since it does contain some muscle fibers. The suspensory is more elastic than the flexor tendons because residual muscle fibers are interspersed in with the collagenous fibers. These fibers are wavy in appearance and when they bear weight, they act as springs, straightening out, and allowing elasticity. It is written in Adams' Lameness in Horses : "The content of muscle fibers is 40% greater in the suspensory ligament of Standardbred horses than in Thoroughbred horses. In Standardbreds, the content of muscle fibers is significantly greater in the suspensory ligament of the hind-limbs, in Thoroughbreds, the content is slightly greater in the forelimb ligament, but the content diminishes when Thoroughbreds are in training. " I find that statement debatable about training causing a decline. Chances are if this decline does indeed happen, it is simply due to aging and not added work.
When injury occurs among the suspensory fibers you get:
1) escape of blood into the surrounding tissue,
2) lymph seeping from damaged lymphatic vessels which causes formation of non-elastic scar, adhesive tissue---not only at the site of injury but into surrounding tissues,
By immediately employing a muscle stimulator (EMS), blood, lymph and other seeping fluids do their work in the damaged suspensory and then they are pumped back out with tissue by-products as nature intended. Nature always intended for the horse to keep on walking! The EMS also keeps any adhesions from forming and tells the injured suspensory how best to repair the damaged fibers in the proper longitudinal wavy pattern. Stall rest is more apt to produce scar tissue, adhesion formation and result in a haphazard put-down of fibers in a weak matrix formation. An electronic muscle stimulator will give your injured horse just the right amount of muscle work without putting weight on that leg or over-doing it.
HOOF TRIM and SHOES
A proper trim on your suspensory damaged horse's hoof is all important, too! Do not raise angles. Try to achieve as normal of angles for your horse as possible, i.e. approximately 45-50 degrees in front and 50-55 degrees behind. You always want to trim for an easy break-over of the affected leg, but avoid raising angles, do it only by squaring the toe and trimming the toe short--never changing the angle. This will foster an easy break-over of the hoof's toe without raising the actual hoof angle. If you have your horse shod, use a half round shoe or some other shoe that will stimulate a clean easy break-over at the toe. I have also put a shoe on backwards in front which means the open part (rear of horseshoe) is on the toe end and the rounded, normal front-end of the shoe is at the back under the heels. Turning the shoe around will give your horse an easy toe break-over plus mimic a bar shoe at the same time. Not a bad configuration on some horses, particularly performance horses. Avoid toe grabs like the plague! Trim the toe length as short as possible. This will also fosters an easier break-over and puts less stress on the front legs. Lastly, it goes without saying that your farrier should use a level gauge on each hoof and make sure that the hoof is trimmed level so that it will land level! Unfortunately, most racetrack platers don't seem to know what a hoof level gauge, toe calipers, or hoof angle gauge are. You need to find one that does!
BANDAGING
Ok, on sports boots and all bandaged support as it pertains to suspensory injury. Again, my opinion, I would stay away from these things when they are applied all day in the stall. I have found that any type of support on the biologic organism will weaken it in the end. It is ok to use bandages in the first few days of a newly injured suspensory though there is even some debate on that premise. Some believe that bandages can cause the seeping lymph and blood to spread into adjoining healthy tissue and cause adhesion formations. That may be true, but with proper daily exercise, this probably is not much of a danger. It is ok to use bandages as a mechanism to apply medication to the leg, but when you try to use it to support the specific ligaments or tendons itself, you are on a fool's errand. For one thing, there is no way that a boot or bandage will protect a suspensory from being over-stretched. Impossible. You have metaphorically a limited-stretchy rubber band next to a bone that is covered by a stretchy bandage or boot acting like a tube. This type of support has absolutely no control in checking how far a suspensory is stretched. It can only apply pressure around the outer margins of the suspensory ligament, not at the origin or insertion points. Bandage pressure can sometimes limit pain in a damaged structure. For instance, if you are hit by a mean brother, you naturally want to take your free hand and apply pressure to this painful spot. Pressure seems to reduce pain. It also controls swelling. So if you are after a temporary reduction in pain or edema, then bandaging can be of some value through its mechanism of applying pressure to the skin and underlying structures. The key word here is "temporary". Some bandaging support may be ok during exercise, but I would try to limit use. Bandaging does limit circulation of both blood and lymph into the injured areas which is not good. We don't want an artificial form of anemia in that area by the use of a tight fitting bandage! The more blood and lymph flow the better, along with proper return. Bandages won't help in this important matter.
I do like the concept of "rubifacients" or counter-irritation. There are also, healing herbs which may be painted on the damaged suspensory that are helpful, i.e. comfrey, plantain, gravelroot, etc. You may make leg paint out of these herbs by soaking 4-6 ozs in DMSO in a glass jar for 2-4 weeks and then straining and painting it on the affected leg as herbal leg paint. You can also make a poultice out of these herbs, perhaps adding bentonite clay and then using it on the ligament at night. And one can use the traditional leg paints of iodine or other irritants designed to increase blood flow and the white blood counts.

Movement (the "M" in Meat)
Using Electronic Muscle Stimulation for Suspensory Injuries
One can buy new, but I tend to prefer the cheaper economy of buying second-hand and would recommend one being patient and acquiring a used EMS unit from eBay or Craig's List here in the USA. Many hospitals, clinics, and professionals are upgrading to newer shinny digital units and trading in or scraping older analog instruments that are just as effective as the new models. Actually, they are preferred for veterinary use as they have easily controlled big knobs! One can save money buying used! I prefer hospital models, but you can get by with the cheaper units designed for home, hand-held use and there are many of them out there to be had. Just be careful not to be misled into buying a TENS unit that is often advertised as a EMS or electronic muscle stimulator when in fact, it really is just a hyped TENS unit designed for pain relief of nerves. If you are patient, you can find good useable professional EMS units for under US$100.00. I have and below are a few examples of my purchases on eBay. There are a number of physical therapy models that employ multiple modes or are Combo units and which not only employ the Russian mode for what we need in EMS but others valuable modes as described at the end of this page. I would lean to buying such a unit. Most used physical therapy units will be for sell without leads and electrodes, but these can be purchased online without too much trouble or added expense. Since we are dealing with the equine who has a hairy coat, the heavier re-usable type of electrodes made of rubber & carbon as pictured below will be the preferred ones. The lighter weight, adhesive ones, common to many human applications probably are not too practical for use in the horse, except maybe below the knee on the thin skin over bones. One can further modify these heavier re-usable rubber ones by inserting a cabinet type knob on to modify it into an easier electrode to use by the practitioners hand to obtain a mobile electrode that can moved as desired in the hand as Charles Strong fashioned with his equine Transeve EMS unit configuration.
I again lean to Charles Strong and his teachings on how to use EMS when treating bad suspensories and bowed tendons. Electronic Muscle Stimulation artificially contracts and relaxes the muscle bundles on which the electrodes are placed. Since I am discussing suspensory therapy here and the suspensory does not directly attach to any muscle bundle, we will rely on the flexor muscles which also work the flexor tendons as the path to treatment of the suspensory. The suspensory apparatus is so closely aligned with the flexor tendons that if you treat one, you will treat both. So the below will hold true for a bowed tendon just as much as a bad suspensory., along with knee and fetlock joint injuries. EMS treatment should start within 24 hours of injury, the same day if possible.
Motor points of the important muscle bundles to place EMS electrode, plus direction of trreament.
Typical reusable electrodes preferred for equine use. The 3" size is probably most handy. These are of carbon/rubber construction and attach to a 2mm pin connectio on the EMS leads.
This is a used RIch-Mar IF-2000 unit I bought on eBay for under $75. It is built like a tank and has the capability of EMS using the Russian Mode along with interfenential current which is also useful. Electrodes were missing, but easily replaced.
Electronic Muscle Stimulation is the best way to satisfy the "M" (movement) component in the above mentioned MEAT protocol (movement, exercise, analgesic, treatment). It will produce movement in the injured part in the safest way possible and should be applied within 24 hours of injury. The region to be treated should be covered in electrode gel which you can make yourself cheaply or at the very least just plain water will work in a pinch. This conducive gel will allow better conduction of the electrical current into the horse and produce a slick surface for the practitioner to more easily slide the electrodes over the hair coat. It is probably advisable for the practitioner to wear rubber gloves with each electrode placed in a corresponding hand while applied to the proper muscle motor nerve point as listed above--if you are using the mobile hand technique or you can tape electrodes to the muscle bundles in a stationary position as is often done in human patients, but I tend to favor the mobile use of electrodes similarly practiced by Charles Strong. Either method can be employed. You just have to move the electrodes to the next muscle position and tape into position which can be some what of a hassle. You will need to find your own individual best way to work with EMS. I am just giving you a broad perspective on principles and techniques. You know what is needed and you can devise your own procedure depending on your equipment and horse.
It isn't exactly rocket science. We want to stimulate the important muscle groups in the forearm, starting at a low amplitude and working up where the muscles are actually contracting & relaxing. Start low to get the animal accustomed to the action and feeling of the EMS and then dial up amplitude. Below are some YouTube videos of a Charles Strong protege working in South Africa using his transeva machine. These videos will give you an idea how the horse reacts and how the machine contracts the muscles. Even though this video is showing the expensive Charles Strong's Transeva EMS machine, you really don't need this exact model. You can make do with the wide variety of EMS machines designed for human use. Just use your imagination a bit and experiment. You can come up with the same effects and results and with a much cheaper price tag!
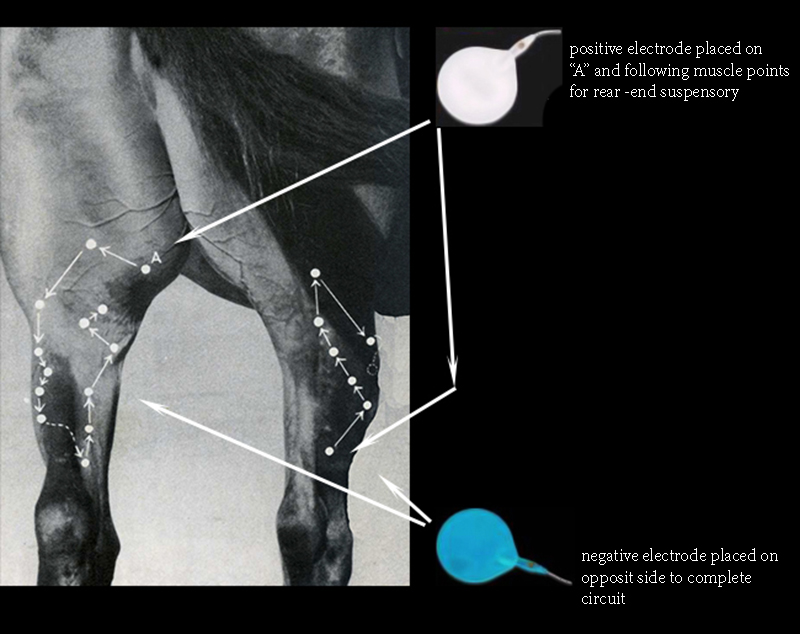
Motor points of the important muscle bundles to treat rear-end suspensories, bowed tendons and the lower joints with EMS.
Charles Strong working on the front forearm which is what is needed for suspensory therapy. Note that it is best to have the leg not bearing weight when treatment is in progress. With the configuration of his EMS unit, he holds the positive electrode in his right hand to the inside of the forearm .
Here is another eBay used unit,purchased for US$210. It is a portable unit (Rich-Mar Theramini 3P) with ultrasonic head. Waveforms available: Quadpolar Classic Interferential, Premodulated Bipolar Interferential, Monophasic (Hi Volt), Biphasic, Russian, Microcurrent.
This is a Combo Stimulator, IF-5000 which I bought on eBay for less than US$50. It is a nice portable, hand-held unit that would be a good alternative to the larger heavier hospital models on this page. Just exchange the light weight human electrodes for the heavier reusable type pictured above. 4 Channels 2 Outputs. Waveforms: Sine Wave & Symm. Bi-Phasic. Modes: EMS, IFT, Russian, Interferential and Sequencing (combo). Frequency: 90-250 VAC, 50/60Hz. Interfential (IFT) Carrier: 5000 Hz. EMS : 1-150 Hz Russian : 2500 Hz. (Carrier) / 50 Hz. (Beat)] This is quite a sophisticated little unit!
Russian EMS Guidelines
Session times and settings should be gradual, but when full contractions are occurring, one must be careful not to fatigue the muscles from over-use when using the 2500 Hz Russian mode. The below should apply to each muscle bundle stimulated in the forearm.
Burst Frequency: 75 bursts/sec
On- time: 10 seconds
Off-time: 50-120 seconds
Ramp-up: 1-2 seconds
Ramp-down: none
Ten contractions per session per muscle bundle, 1-3 times a day, until healing is achieved.
Do-It-Yourself Conductive Electrode lubricate or Gel
There is nothing magical about conductive electrode gel which when purchased over-the-counter can be quite expensive. Tap water can be used in a pinch. In most cases, plain old salt is the key ingredient that will cause most all liquids to conduct electricity i.e. a little table salt into aloe Vera gel, glycerin, plain salt water with some soap added, etc., all can make adequate conductive lubricate. Some added soap will help the lubricant solution more easily allow electrodes to slide over the hair coat. Read the conductivity of the electrode gel by placing the two electrodes of a multimeter about one inch apart in the gel. If the resistance of the gel is too high for your purposes, add more salt.
Conductive gel materials:
1. Water, 1 cup
2. Salt, 2 tablespoons
3. Flour, 1 cup
4. Bleach, just a drop
1. 100 ml of aloe vera gel
2. 1 tablespoon (20 grams) of salt
1. K-Y jelly
2. salt
An interesting, useful formula for a water soluble grease or gel depending on how much corn starch you want to add to glycerin can be made quite easily by heating glycerin and dissolving up to 2 spoons of corn starch into it. This makes a great high vacuum grease (full two spoons) to seal glassware needing to be air-tight and can also make a nice conducive gel by adding a bit of salt to the formula with less corn starch.

Exercise (the "E" in MEAT)
Now to the "E" in the MEAT protocol which is exercise. One might think that movement and exercise are one of the same, not so in this case. Exercise will be considered actual out-of-he-stall exercise for the racehorse where he is in motion and bearing weight. Like movement, exercise needs to be started as soon as possible in the suspensory injured horse. It will help prevent adhesion formation and stimulate proper healing. Just plain shed-row walking should be applicable within days of an injury at the very least and should not be neglected. Electronic muscle stimulation is all well and good and a life-saver in the early days of an injury, but it is no substitute for actual animal movement under-weight doing work. However, continue your daily EMS stall work in conjunction with exercise until you consider the patient cured.
There is no cook-book recipe for me to tell you when, what type or how long to exercise your injured horse. It really depends on the degree of injury and your horse's individual response to that injury on how best to administer a rehabilitation program. I guess that is why one pays the big bucks to the professional trainer, but many times these professionals seem to have less of a clue than you would. The key is to observe some common principles, have a good handle on how sore your horse is and go from there with a graduated exercise program that will get your horse moving without causing further damage to the suspensory. As I wrote above, exercising your horse is a delicate dance between giving just enough exercise to stress the injured suspensory showing how best to heal the ligament without causing further damage. A horse can show some nodding and it is still all right to move him, some pain is acceptable but again, you will have to be the judge with how much your horse can take. For the most part, walking either by lead chain or under saddle will be permissible very soon. You will have to evaluate after each daily session the next morning what to do during the new day---backing off, maintaining, or increasing work loads. You will have to observe how easily your horse moves. You will have to understand the suspensory's anatomy and monitor it carefully with your fingers every day as well. You will have to carefully palpate the ligament from knee to ankle and use ankle flex tests to try to gauge how your horse is progressing. If he seems to be coming along nicely, continue to increase work loads from walking under saddle, to trotting, to cantering, to galloping, etc. You basically have to start from scratch and allow time and your treatment to affect a healing of the suspensory fibers, adding the right slice of work to tell your horse's system how best to heal.
Diagnostic Palpation Procedures:
1) Start up at where the suspensory ligament originates on the first row of knee bones. Place finger pressure in that region and see if you can obtain a painful response. Do this with the suspected leg flexed off the ground. The usual painful reaction is the horse withdrawing, attempting to get away from the pressure. Always compare the suspected injured leg to a sound leg to better gauge if the pain is from actual tissue damage or is more the nature of that individual horse.
2) with the leg still off the ground, take your thumb and finger and pinch the suspensory tendon from the knee down toward the sesamoids. Note any painful response and degree of pain.
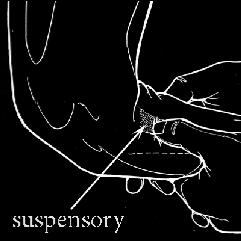
3) The most common suspensory damage occurs in the distal third of the ligament near where it branches off around the sesamoids--one branch or another. The ankle flex test will elicit pain from injury in this area. Also, applying finger pressure as illustrated below over the sesamoids can denote a newly damaged suspensory though both of these mentioned tests can easily involve pain from other damaged structures situated in the region in addition to the suspensory.
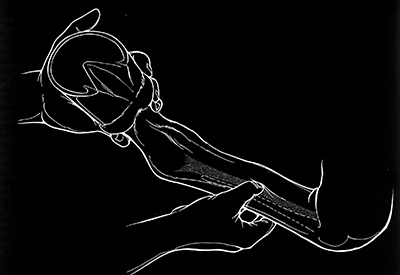
Finger pressures all along the ligament.
Finger pressures on he outside of the sesamoids where the supensory attaches with foot off ground.
Analgesics (the "A" in MEAT)
As I wrote earlier, this is one aspect of the MEAT program, I would avoid and not employ. A trainer needs to know when the horse is hurting and how much. Analgesics tend to mask that response. I do appreciate why it was put into this program in the first place as movement and exercise are considered so important that the animal must be made to move as soon as possible and pain killers would help this, but I have found, they are not needed. Analgesics can cause more problems than they are worth. The use of anti-inflammatories (bute, etc) are an absolute "no-no" in my book, retarding healing!
Treatment (the "T" in MEAT)
The good news, suspensory ligament damage is much easier to heal than bowed tendons, but that doesn't mean it will be easy. The blood supply in the suspensory is much more limited than in other structures though it tends to have a decent lymphatic system. The traditional routes of suspensory treatment often found in the race track's shedrow were hours of tubbing in both hot and cold waters, the painting of various counter-irritant leg paints, blisters of all degrees of strength, sweats of various types, etc. I have used all of these to varying degrees of success. I would like to suggest some pit-falls to these old time standbys as well as newer more efficient suggestions.
First off, the endless icing, tubbing, hosing that is often seen on the racetrack in not only suspensory injuries, but all types of leg injuries: To this I say, "The road to hell is paved with good intentions." Mostly this is all a waste of time, natural resources and a groom's hours. Cold therapy is only beneficial the first 24 hours of an injury with the goal of slowing down what can sometimes be run-away inflammation. Actually, cold should only be used in the first hours and by the time the first day is over with, it is of little use. If edema is already present, it will not do any good at all even during the first day or hours. I once worked for a Hall of Fame trainer that was rabid about using pounds of ice on his injured horses as most of his peers were also apt to do. Some barns even had commercial ice machines right in their shedrow for easy access for the grooms! This trainer was involved in a racing accident one afternoon, and I heard it directly from his wife that he soaked that evening in a nice hot bath. No ice for him! This innate response to one's own injury should be pretty telling on the true value of ice and cold therapy for injuries! As far as ice being used to numb pain, I view this as almost criminal. I have seen plenty of trainers try to freeze their horse's legs or hooves in ice water before going to the paddock to race. Terrible and an abomination! What human athlete ever used this method to race better? I would like to see some of these so called trainers freeze their legs and feet in ice water and then go out and try to run! Even if this procedure did work for any length of time which it does not, why would you want a horse numb to pain at the risk of doing far more serious damage? Hours of hosing an injury is another common racetrack procedure. It is very common to see a groom with his horse on a wash rack or out front sitting on a bucket with a water hose splashing on his horse's leg. What a waste of time though I am sure the groom is glad to be able to sit a spell. The tap water is not cold enough to make any difference and as for as a possible massaging action of the water lapping on the injured part, that is highly unlikely to be of much value either. It may look impressive, but if you think much on the subject, not very logical on all counts.
Various leg paints, working blisters and severe blisters have been used for tendon and ligament problems for many years in the racehorse business. These are mostly of the counterirritant variety that can contain varying amounts and combinations of iodine, mercury, cedar oil, camphor, oil of wormwood, oil of organum, mustard seed oil, croton oil, etc. These extracts are mostly carried in ethanol and/or DMSO bases and is designed to stimulate blood circulation when painted on the affected region. The only problem is, it doesn't stimulate a return mechanism. Its a one-way street if you only stimulate blood flow without pumping it out. Used by itself on a horse at rest is not particularly good. You will get an accumulation of blood and fluid from this type of stimulation and stagnation could likely occur opening your horse up to adhesion formation. What is known as a "working" leg paint is useful as you use these types of light blisters while at the same time exercising your horse. The paint will stimulate blood & lymph flow and the simultaneous daily exercise will stimulate the pumping away of the blood, lymph, toxins. This is a combination that should be present when using a counterirritant! I tend to like iodine in my counterirritant leg paints and there are all types of iodine formulas. Rite's knee & hock paint is a pretty useful formula which I have used it for years. For its formula, go to my leg paint web-page. I would stay away from the severe blisters that particularly contain cedar oil and mercury. I have seen and used my share of these while working for some old timers, but I have long felt that this degree of blistering does little therapeutic good. This is one aspect of our racing history where our forefathers probably went wrong. One should avoid tissue destruction that is seen in these types of blister applications. If you have to use a neck cradle on your horse as is often the custom when using a severe blister then something is inherently wrong with the treatment! Same holds true for using a hot firing iron. Even though our old time horsemen swore by the effectiveness of firing a horse, it is just another out-cropping of the human tendency to believe "more is better". I never fired a horse in my life that I trained, nor used a severe blister. I feel I missed nothing in not using them. I always preferred a light blister that only would affect the skin by stimulating some crusty scurf formation after a few days of application---nothing more severe. In most cases, I don't think you will need to apply a counterirritant paint to a bad suspensory but every case is different and at times, one may want to stimulate an increased blood supply to the injured ligament. If so, then use a counterirritant.
I do like leg paints, but I prefer herbal leg paints that stimulate healing. There is none better than comfrey! Comfrey is an amazing plant that has gotten a very bad rap in the last 50 years which is at odds of its hundreds of years of dedicated use by herbalists of many ages. A comfrey leg paint is very healing and if you are dealing with an open wound, it can actually heal the outer surface faster than one should, leaving an infection inside. This is one of the dangers of using comfrey. It will heal the skin over faster than it should preventing drainage. In the suspensory, one does not have to worry about this aspect. A simple formula for a comfrey leg paint can also be seen on my leg paint web-page. I would paint the bad suspensory every day using a toothbrush type of applicator. It is an amazing healing herb! A colloidal silver, castor oil, DMSO leg paint is another formula very healing, and I particularly recommend this when using HVPC therapy discussed below.
There are a few electronic medical modalities that may also be useful in treating suspensory injuries besides the above mentioned EMS. Electronic muscle stimulation is designed to indirectly aid in healing the damaged ligament by contracting & relaxing the muscle bundles which stimulate blood & lymph flow to the region. There are other electronic forms that actually may induce healing directly of the damaged tissue. If you are lucky enough to find a used therapy unit that contains these forms, then by all means use them. The waveforms that may be of value are 1) Quadpolar inerferential, 2) bipolar interferential, and 3) High Voltage Pulsed Current (HVPC). I discuss these in-depth on my Electro-medicine Part 1 page. It is thought that application of these forms will aid in pain relief, stimulate the meager muscle fibers found in the suspensory, increase blood flow, reduce edema, stimulate tissue healing and repair. Below are some suggestions where to place the electrodes using these protocols.
Note, there are all possible areas of the suspensory that can be damaged; however, I will only suggest where to place the electrodes on the more common branch injury found near the sesamoids. Also, be aware that since we are placing electrodes on areas of the leg devoid of muscle tissue, below the knee, that one may have to resort to the smaller more flexible human type cloth/carbon TENS electrodes which are more flexible and lighter weight. Make sure you apply plenty of electrode gel into the hair coat and that each electrode is securely fastened to the below areas by athletic tape and/or elastic bandages to maintain a stable position during treatment sessions.
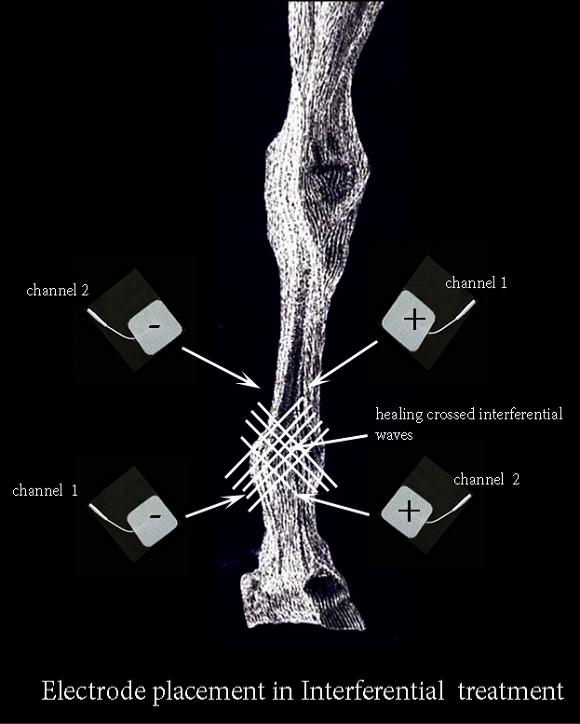
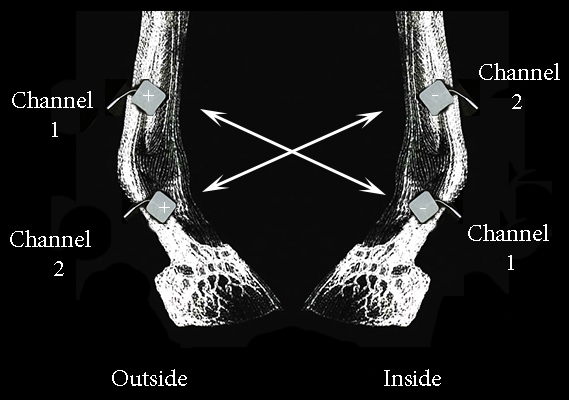
Above is a suggestion where to place the four electrodes on the leg to best treat the injured branch of the suspensory. The quadpolar interferential wave form requires two channel leads with two electrodes per lead for a total of four. They are placed on the leg to criss-cross which is what generates the healing IFC waveform. The below illustration shows outside and inside side-views of the front leg where two of the four quadpolar electrodes are placed on each side o0f the leg--crisscrossing the current channels.
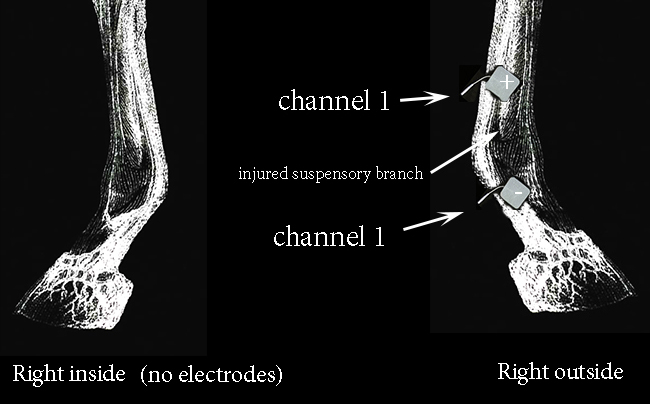
Bipolar Interferential current is another form that could be of use in healing an injured suspensory, but unlike quadpolar previously discussed, this method uses only a one channel lead with a total of only two electrodes to be placed on one side of the injured area. Below is an example where to place bipolar electrodes on a damage branch of the suspensory. This generally is not as deep penetrating as the quadpolar, but may be of value.

Lastly, an electro-therapy current form with many names such as High voltage pulsed current (HVPC), Hi-Volt or Monophasic can also be used to good benefit. Depending on what you want, the electrode placed on top of the suspensory should either be positive or negatively charged. It is thought that if you put a positive charged electrode over the injury that it will heal best during the initial phase, then the polarities are changed in the second phase of healing to negative where there-after polarities can be exchanged, day to day.
I feel this waveform may be the most helpful in stimulating a healing response because of the research don't by Dr. Robert Becker on his work with silver ions and electro-therapy in joint regeneration. You can read in-depth about his work on my arthritic joint page. He found that if silver ions are present along with a low level electrical charge, the silver ions associate with cells in the injured region, particularly fibroblast & epithelial cells, resulting in de-differentiation of these cells into embryonic cell types. It is these stem cells that can aid in regeneration of the suspensory. I would suggest painting the damaged suspensory with a colloidal silver & DMSO gel or lubricant to take the place of the normal conducive electrode lubricant. This would place silver ions over the damaged suspensory site and with the aid of HVPC and DMSO, help drive the silver ions into the suspensory aiding in healing. You can read about Colloidal silver on my CS webpage and make a simple CS paint by simply mixing a 50:50 solution of DMSO and Colloidal silver. Paint it on liberally before applying both electrodes.
As illustrated below, place the positive electrode directly over the suspensory damage while placing the negative electrode over the opposite suspensory branch on the other side of the leg:






Suspensory Injury Protocol Summary
1) Use EMS as soon as possible, preferably the same day and continue until a healing is achieved.
2) If this is a typical racehorse with a long toe, low heel hoof trim, begin trying to correct hooves to natural angles of 45-50 degrees in front and 50-55 degrees behind with toes trimmed as short as possible to aid easy break-over. However, only change the angle no more than 3 degrees at any one time until the horse can become accustomed to it. Also, get rid of any toe grabs.
3) As soon as the horse is able, start exercising outside of stall with gradual incremental hand-walking, walking under saddle, onward to track work---monitored daily and guided by how the suspensory is healing.
4) Treatment may take many forms, but I have found painting with a comfrey DMSO leg paint to be very helpful. One can also use a colloidal silver DMSO paint combined with HVPC to try to stimulate a stem cell type regeneration. One can also use other electro-therapy modalities such as quadpolar IFC and bipolar IFC. It goes without saying, depending on how the healing is coming along that one can use various counterirritant type paints, sweats, poultices, and whirlpool tubbing in hot water to aid in the healing process. It is doubtful that cold therapy will be of much use after the first few hours of injury. Bandaging should be used sparingly, mostly to help apply medications.







