James R. Rooney, DVM writes of one interesting observation in regard to complimentary lameness as observed in the thoroughbred. He writes that it is a well known fact that lameness causes lameness, that a minor lesion can cause a major lameness. I agree whole heartedly. He also writes that in the running horse, one will mostly see the following:
1) Lameness in one foreleg leads to lameness in the other foreleg.
2) Lameness in one hindleg leads to lameness in the foreleg on the same side.
3) Lameness in foreleg does not lead to lameness of the hindleg and the lameness in one hindleg does not lead to lameness in the other hindleg.
The Rotary Gallop or Run
Unlike the previous transverse gallop, this form of gallop is rather rare in the equine and can only be seen in certain instances, primarily at the first few strides when a horse breaks from the starting gate or in lead changes. The rotary gallop is commonly seen in other animal species, i.e. the dog, deer and others.
----------------------------------
Secondary Lameness
by James Rooney DVM
It has long been known that lameness, pain in a leg, can and often does lead to lameness and pain in another leg. As an adage: lameness is a cause of lameness. In the 1960s I called this second site of pain "complementary" lameness. That was not original with me, I'm sure, and is not really correct in any case. Perhaps secondary or consequent lameness would be better; at any rate I shall choose consequent
Of more importance, however, is defining what we are talking about, systematizing the observations, and seeing if the system we develop stands up to empirical test.
1. If a horse is lame in one foreleg, it tends to shift weight bearing to the other foreleg and to the contralateral (diagonal) hindleg. A clinical sign of lameness of, say, the left foreleg (LF) is that the head and neck move up when that lame left leg is bearing weight and move down when the right foreleg (RF) is bearing weight. This is known as nodding. The reason for the nodding is as follows: When the neck is raised (dorsiflexes) there is reflex extension of the leg in support at that time. Thus, with the LF lame and in support - bearing weight - the horse raises the neck, which induces extension of the LF. With extension there is less movement of the joints of the leg and, so, less pain since much of the pain of most lameness is caused by movement. In your own case, if you hurt an arm or leg, you try not to move it because that causes greater pain. Simply put: if it hurts don't move it.An additional sign, usually less obvious, is that the horse will carry the head and neck slightly curved around toward the lame leg.
2. The neck is curved around toward the lame foreleg because, again, this induces reflex extension of that foreleg and, so, reduces pain. I hasten to note that these reflex extensions (and many more) are all part of the normal locomotion of the horse. We are here considering them only in relation to lameness.
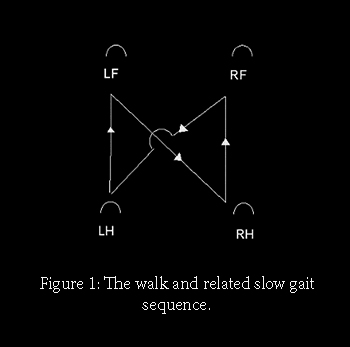
3. As mentioned above, if a foreleg is painful enough, the horse shifts some of the weight-bearing to the contralateral (diagonal) hindleg as well as to the contralateral foreleg. Say the horse is lame in the left fore (LF). We start the horse walking with movement of the LH. The LF moves next, then RH, then RF and back to LH again, Fig.1. Thus, RH is always the next leg to bear weight and move after LF. (Start with RH and you will see the same thing.) One may propose that since RH is next after LF and LH after RF, that when either fore comes to the ground and pain is experienced, the horse shifts weight as quickly as possible to the next leg in the normal sequence - the contralateral hind.
That sequence is, of course, true for the walk and related slow gaits. At the trot if the LF is sore, weight can only be shifted to the RH since that is the only other foot on the ground. Similarly for RF sore and shift of weight to the LH. The gallop sequence, diagonal or round, is different, and we shall try to deal with that later. In any case lameness is evaluated at the walk and trot, and we concentrate on those gaits.
I must, however, take a moment to consider the lateral gaits, so-called: rack, pace, single-foot, etc. At the pace, for example, if LF is sore, the next leg in sequence is not LH but RH, and the contralateral principle holds.
It would be nice, very nice, to be able to extend these observations to primary lameness of the hindleg and secondary or consequent lameness of a foreleg(s). Going back to 1. we saw that reflex extension helps to alleviate pain in a leg. If LH is sore, reflex extension should help, and such reflex extension is achieved by the horse lowering the neck (ventroflexion). In the real world, unfortunately, it is difficult and usually impossible to perceive such movement. There is no real and easy explanation for that. One factor is that lameness of the hindleg (e.g., spavin, sacroiliac arthrosis) is almost invariably bilateral - both hindlegs affected. With pain shifting back and forth between the two hindlegs it is virtually impossible to distinguish significant ventroflexion of the head and neck related to one leg or the other. It is generally true that horses lame behind tend to carry the head and neck lower than usual but, again, that is very difficult to appreciate in most cases.
We have been considering this from the viewpoint of diagnosing the site of lameness. Of equal, and perhaps greater importance, is understanding why a horse lame in one leg becomes lame in another leg. In brief, in summary, all one has to do is to examine the gait sequence for walk and trot as in Fig.1; the next leg in the sequence after the lame leg will be the site of consequent lameness.
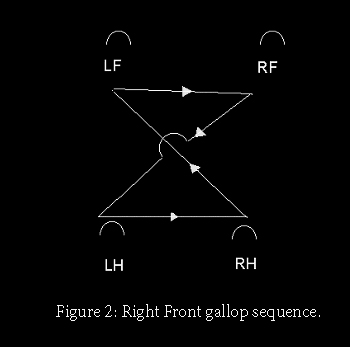
Gallop
The gait sequence for the diagonal gallop is shown in Fig. 2. We take the horse on the left (LF) lead with LF sore. The sequence is: RH-LH-RF-LF. That is obviously not a good situation for alleviating pain, the lame LF being in sole support. The horse shifts to the RF lead with the sequence: LH-RH-LF-RF. LF is now in the diagonal with RH and, therefore, sharing the weight with RH rather than being in sole support. IF there is to be a consequent lameness, it should be in RF and/or contralateral in the RH. In the real world, once again, one more often sees consequent lameness in the contralateral foreleg and not (apparently) in the contralateral hindleg. Consequent lameness of RF occurs because RH leaves the ground a bit before LF, so that alleviating pain in LF requires a quick shift of body weight to RF - the next in line in the gait sequence just as at the slow gaits.
All these bets are off, of course, if one considers the round gallop. I shall leave that to the reader, if interested, since it is an uncommon situation but can be worked out using the gait diagram.