The medical establishment in the 1920s and 30s were aghast at the use of HCl acid as used by Ferguson and Guy. A lot of negative editorials appeared in the medical journal, JAMA. Most cited that hemolysis (destruction of the blood cells) was the main reason to avoid this experimental practice. Dr. Ferguson's response:
"Since the J.A.M.A. has so frequently given the opinion that injection of 1-1500 hydrochloric acid was dangerous in the great hemolysis following its intravenous use, I decided to look for danger in this case, which I had done many times before. So I gave 10 cc intravenously, 1-250 putting the remaining drop of blood in acid solution on a microscope slide at the finish of the administration of the injection. Nowhere could one see any change in the contour of red cells. According to the opinion from Chicago (JAMA), I should have seen destructive change, but I did not."
Dr. Ferguson discovered that injecting dilute solutions of Hydrochloric acid could result in many infections being overcome resulting in successful recovery. This was back in the day when our modern antibiotics were yet to be discovered. Penicillin only came onto the scene around 1940. Ferguson and Guy were doing their work in the 1930s and earlier. Dr.Ferguson is an interesting chap and to understand how he developed this therapy is informative. While working with mercury and arsenic compounds around 1913 as injectable substances in the form of salicylate of mercury and Salvarsan, Ferguson discovered that both were extremely effective against skin infections. Before I lose you on this one, note that the use of mercury and arsenic were very common during this time period, though very much detested by many people because of accompanying side-effects. Needless to say, modern practitioners are shocked that mercury or arsenic were ever employed, but it cannot be denied that these two toxic compounds did cure in many conditions. The thing was, both of these substances had never been given as injectables until just recently in Dr. Ferguson's career. He started injecting salicylate and curing patients. Healings were promptly stimulated by these injections. He later practiced in the US Army during WW1. Though he was assigned to an administrative military office, he occasionally treated stubborn skin infections successfully with injectable salicylate. After being demobilized in 1919, he joined the American Red Cross for work in Siberia. He again found many opportunities to use his injectable salicylate on slow healing wounds after amputations, furunculoisis and unknown infections--all with surprising results as he writes. Later he was ordered to Albania to investigate a malaria epidemic. Once there, he treated specific malaria cases with injectable saliyclate and this time also Salvarsan. He felt that his treated malaria cases when compared to traditional treatment with quinine, cured faster and was superior. He wrote: "There appeared to be no reason for such results but I felt that there was some unusual explanation that my mind was not yet able to grasp."
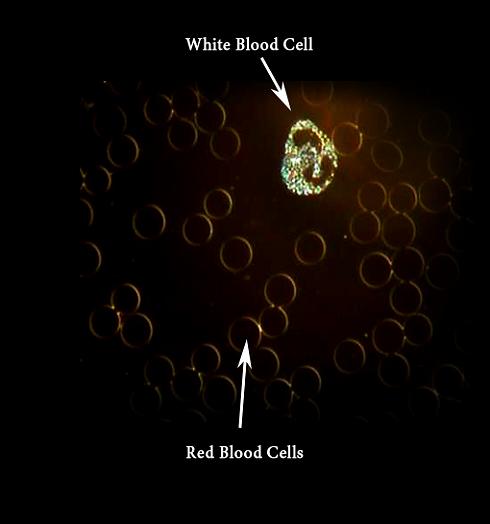
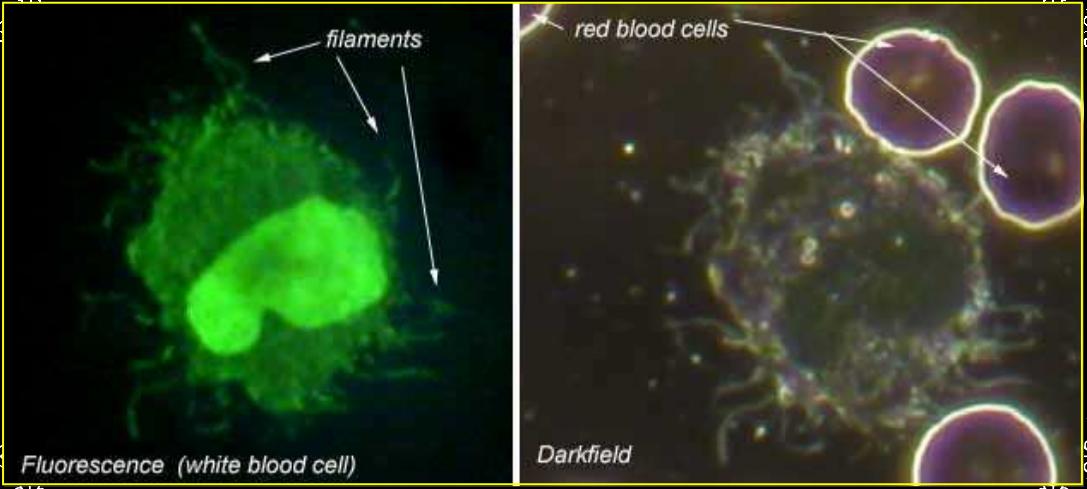
In 1923, a U.S. Consul in England was suffering from an infection of his axilla glands which would not heal after five weeks of treatment. Dr. Ferguson was called in and immediately resorted to his tried and true salicylate injection resulting in the infectious lesions immediately responding. The dressings were thrown away the next day! Finally, upon consultation with another physician on the mystery of why salicylate seemed so effective, Dr. Joe Doyle came up with the possibility that salicylate injections stimulated the white blood cells resulting in the relatively new concept of immune response of phagocytosis, the engulfing of microbes by phagocytes. Dr. Ferguson immediately took this insight and started experimenting with blood counts and injections. In cooperation with a pathologist, he injected himself with salicylate mercury. Ferguson's white blood cell count before the injection was 9000. Twenty four hours later another wbc count was completed which showed 18,600. Other similar experiments were completed with volunteers with exactly the same results of increases in white blood cells. Further more, Ferguson discovered that white blood cell stimulation was not just limited to salicylate, but injected novarsenobillion, quinine, bismuth, milk and plain old distilled water all stimulated the white blood cell count upon injection. Rightly or wrongly, Dr. Ferguson concluded that "...all injected agents derived their powers from a stimulation of natural defensive forces of the body." Certainly, this was an outlandish conclusion for the times and even today, but there may be some truth to this! The power of doubling the white blood cell numbers should not be overlooked, even in these modern times!
Shortly after this work, Dr. Ferguson happened to run across a used copy of Metchnikof's Immunity in Infective Diseases in an old book shop in Rotterdam. This text offered Ferguson the scientific proof that he was on the right track. He was elated and in 1923, he journeyed to the Public Health Service in Washington DC with news of his discovery. He was told in no uncertain terms that his ideas were too revolutionary and that more tests were needed, at least 10,000 cases. Ferguson was disappointed in this reception. He also found resistance to his new discovery back in England. The prevailing thought was that antibodies were the prime immune reaction to fighting infections, not the white blood cells. It was felt that increased white blood cell numbers were only an indication of infective disease being present, nothing much more. It had been proven during this time period that both Mercury salicylate and arsenic were not specific germicidals for syphilis alone, yet both seemed to benefit a recovery in this disease. The problem was, no lethal effect on bacteria could be shown in the blood stream by mere contact with mercury or arsenic. Also, Metchnikof proved over 25 years previously that a culture medium containing anthrax, cholera and other similar harmful organisms were not affected by accepted toxic substances like mercury or arsenic. One can only conclude that it was the increase in white blood cells from the body's immune system that was the effective determinant to fighting infection, particularly in the affect of mercury or arsenic on syphilis and not a germicidal affect.
In 1926, Ferguson started treating gonorrhea at the Hillman Hospital. All cases coming to the clinic were treated solely with injectables to stimulate the white blood cell counts. 350 cases were treated with excellent results. Of these 350, one third were acute and cleared up in 5-6 weeks. Most of the chronic infections with histories of 6 months to over 5 years cleared up after about 40 injections. A 1% Mercurochrome solution was being injected at around 8-15cc with good results but the white blood cell count was not maintained as well after its use as with arsphenamine. Also, white blood cells were stimulated with intramuscular injections of salicylate and bismuth. During this period of using mercurochrome and arsphenamine, Ferguson saw too many reactions in his patients to make him happy with their continued use. By chance, he received a card in the mail announcing a lecture by a Dr. Granville Hanes on his new treatment for pruritus ani, and he attended that meeting. Dr. Hanes lectured how he injected Hydrochloric acid at 1:3000 dilution under the lesions of this anal infection for very consistent good results. Dr. Ferguson experienced one of those Eureka moments! Hydrochloric acid was the substance he had been looking for all of these years! Ferguson knew that Hanes was stimulating the white blood cell count resulting in his successes. Dr. Hanes had attributed the use of HCL to some unknown factor of the acid. Ferguson immediately took this knowledge back to the lab and found that Hydrochloric acid injected at 1:1500 in 10 cc doses, intramuscularly, produced a white blood cell increase of 2500-3500 in one hour. He felt that Hydrochloric acid was completely safe with no contraindications. After all, it was a naturally synthesized body acid produced in the stomach. He immediately started further testing.
He quickly determined that the problem with intramuscular Hydrochloric acid injections was the pain for the patient. Dr. Ferguson decided that there was no reason why this HCL solution could not be given directly into the vein and he injected himself and two others. He quickly found that an intravenous injection did no harm, nor was there any reaction and it was painless. Thus, began his years of clinical practice with injectable Hydrochloric acid in various strengths, mostly 1:2000 to 1:500 at 10 to 25cc amounts. It has proven uncannily effective against all sorts of infections, severe pneumonias, septicemias, malaria, typhoid fever, pain relief, tetanus, smallpox, venomous bites, anthrax, and some cancers. For more detailed case studies, one should study their books. I won't go further into Ferguson's successes.
I first tried dilute hydrochloric acid injections on a young goat that had decapitated a front hoof in a fence accident several years ago. I mainly wanted to see if HCL could keep the amputated digit free of infection and how the goat tolerated HCL injections both IV and IM. I treated the animal for approximately two weeks in a dirty barn environment and found the amputated limb to be surprisingly infection-free throughout. The nanny was soon sold to market which ceased my experimentation of this particular subject. This nanny showed no ill effect from intravenous injections of 1:2000 dilution of Hydrochloric acid in dosages up to 10cc. I did a few intramuscular injections and as I suspected, the goat showed symptoms that this route was rather painful, stinging. If I planned to do many IM injections, I would mix the dilute HCL with a local anesthetic as recommended by Dr. Ferguson in his text for a more humane administration. It could also be given subq (subcutaneous).
My second subject was a beef type calf which was dropped during a snow storm on Feb. 28, 2009 to a mother that was "dry". He was soon taken off the old cow and bottle fed with frozen colostrum and formula. He soon developed pneumonia with fever and labored breathing, characterized by thick mucus exudate from both nostrils. Initially, the broad spectrum antibiotic, Baytril© was injected with improvement. Two weeks went by with the calf again developing pneumonia. When I saw him, Baytril had just been given a second time and he was laying in the sun, head and neck extended forward on the ground with labored breathing. He would curiously open his mouth every 10 seconds or so in an opening and shutting motion with gulping of air. Edema was seen in all four ankles with the left hind the most severe. His temperature was taken which showed 106*F degrees (normally approx 102*F). To the best of my experiences of the past, this calf showed all indications of being close to death. There was no improvement 3 days after the second round of Baytril. However, he did exhibit an encouraging strong appetite and sucked his bottle well when encountered.































.jpg)
.jpg)


